воскресенье, 2 октября 2011 г.
понедельник, 15 августа 2011 г.
Why QL in spasm?
воскресенье, 14 августа 2011 г.
Последние выводы о состояниии my mysculoskeletal system
-> Trunk right rotation L4 on L5;
Left on Left Sacrum Torsion; L5 goes with sacrum
Left Leg functionaly Short->Right Inominate Anterior Shift with Ant Rot -> Change in relation Inominate-Hip-> Right Hip Looks Like Externaly Rotated-> расслабление TFl/Ant GlMed on Right
->Hypertonus Biceps Femoris R

Right: Superior part GLMax - Immobilization Inability of Contraction
cause restriction of antagonist myofascial unit(changed ralationship R Inominate R Hip)
Action: Hip Hyperextention last Phase
inable to do it in Sagital Plane. Shift of movement plane. Forced Abduction & External Rotation
Left: Lover Part
Weakness Inability of power contraction
test: good morning exersice on one leg
Not Engaged/Participate in low back extention from bending position->
Inactivation Multifudus &Part of Erectors probably Iliocostalis that conected with Glut Max (neigbours in kinetic chain)
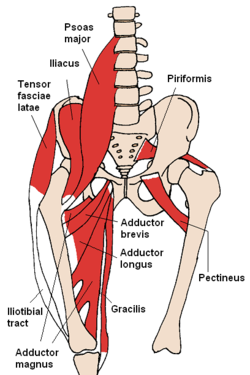
There is two portions of Glut Max.
Superior: originates at the posterior sacrum, ilium(superior gluteal line); attaches to the gluteal tuberosity of the femur;
Inferior: originates at the posterior sacrum , ligamentous(sactoruberous, iliosacral lig) sheath; attaches to iliotibial tract.
Glut Max Effect Sacrum Angle - increase Pelvic Tilt
 3) Расслабление Glut Med Ant Part Right
3) Расслабление Glut Med Ant Part RightTest: One leg standing position hip slightly extended & internaly rotated Inominate Shifted Posterior (Like as Opposite leg going to make a step Hip Flexed with Inominate Anterior Translation)
=> Left Inomminate Drop
Left Glut Med Post, Piriformis External Rotators "останавливают падение"/останавливают Shift
Assist Gl Max As Stabiliser in Hip Extention
Inability to Internaly Rotate From Leg Extended Position->
Inability to stabilyse Leg (antagonist for Gl Max) in Leg Extension->
Inability Gl Max To Forcefuly Contract
4) Short Hypertonic Ilia-Psoas Left
Reason: a) massage work Using Right Arm more Long Stroke With Right Arm Create Rotary Moment
b) Hypotonic Left Erectors Trunk Left Rotatores, Left Multifidi
c) Hypotonic Left Internal Obliques
d) Posterior Pelvic Rotation : останавливает rotation when sitting
5) Hypotonus Internal Oblique Left
Reason: Judo Right Trunk Rotation Left External Right Internal Obliques Overdevelopment
Inability to contract Why: restriction of left trunk rotation Iliapsoas(pulls low back ventral inferior & right rotation- lock vertebra in Fl Sl Rr)
6) Hamstrings Hypertonic
Why: Glut Max Inability of contraction->Hamstring Facilitate
7) Hip Rotatores:

Quadratus Femoris; Obturator Internus- расслабление этих мышц может привести к diclocation of femoral head & changes in hip-inominate relationship. Probably can cause Inominate Abduction.
8) Sartoris
9)Grasilis Adductor Longus vs Adductor Magnus
Adductor Magnaus and Inominate Adduction
10) Rectus Abdominis & Internal
Int Obl Inablility To Contract
11) Walking Leg Knee Hyperextention Phase- Hamsting
Knee Hyperextension Gastrocnemius
Popliteus Plantaris Knee Closed Pack Phase
TODO: Corrective Exercise Program/Protocol
суббота, 13 августа 2011 г.
четверг, 4 августа 2011 г.
Inhibited TFL. Остановленное падение
Contrlateral side: Leg goes in internal rotation, pelvis goes shifts posterioly
Pelvic girdle rotates to the left -> spine ralatively rotated to the right
*L5 goes with sacrum rotates to the left => L4 rotated on L5 to the left
понедельник, 25 июля 2011 г.
пятница, 22 июля 2011 г.
пятница, 8 июля 2011 г.
Tricky TFL mechanic
A:
Hip flexed:
internal rotation
Hip extended:
ext rotation
Ant: Glut max superior part
Hip protraction stance leg neutral position standing on one leg
Hip abduction open chain
Restrict Close chain hip abduction (protraction) ...
- Push into ground with opposite inominate elevation
Antagonist glut med min contrlat QL, unilat costalis
Sent from my iPhone
четверг, 7 июля 2011 г.
Passive insuffitiency or just switch of kinetic chain
Hamstring rectus femoris vastus lateralis***
glut max vastus medialis grasilis adductors
Odna kinetic chain perehodit v druguy
V norme perehod dolgen bit plavnii and stable
Sent from my iPhone
Build your ass web site
Harina kak model for web site - build your ass
Sdelat paru video on YouTube kak activate ass
Why you need ass why we like ass
Sslki na knigi authorities
Posmotret kak bidet poseshaemost
Sent from my iPhone
Gde tonko tam vibrate
Ex: Inhabited latisimus dorsi =>
Uvelichenii kifoz
Low back: tigth spinalis multifidus=>
Increased arch
Tight iliocostalis QL => decreased arch
Konechnosti
Sustav stabiliziruetsya s protivopoloGnih storon kranoalno & kaudalno
Ex
Hip tfl adductors
Adductors gluts
Glut max grasilis vast lat
Vast lat peroneus
Sent from my iPhone
Closed chain MET; bones as soft tissues
Piriformis syndrom
Posterior pelvic rotation-> periformis compression->
Sitting -> stress on Piriformis-> shortening Piriformis->femur abduction-> weight shift-> glut med stress->shortening->inominate abduction
Press
Hold
Decrease pressure until tissues don't push u out
Hold
Push or pull muscle energy
Engage joint cheers dosednii sustav
Hip cherz knee
Knee cherz ankle
Ankle cheers knee
Force goes throug vspomogatel'nii joint blizko k osi kosti
Ex. Push into table with arm extended sitting poss chest open
Compress attachment mus in short rom
Elongate
Passive stretch
Active close chane stretch with release
Breathing
Exhale relax act move in short rom
Fixate very steady joint
Pos release
Inhale move in long rom
Continue....
Note: deistvuet ocher' efectivmo
Ispolzpvat posi iz yogi
Shiatsu
Preassure with single finger
Sensational phenomen
Press on bone
Immediate effect
Sent from my iPhone
среда, 6 июля 2011 г.
Yoga - streching with stability
те одни мышцы растягиваемые, (1 група мышц) ставятся в lengthened position уже из-за самой позиции
при этом другие мышцы назовем из антагонисты (вторая группа мышц) оказываются в shortened position
contraction of antagonist - обеспечивает невралогическое расслабление lengthened muscles, дополнительное механическое растяжение, стабильность сустава без которой тело будет "сопративляться" растяжению 1ой группы мышц.
Надо учить Bones Landmarks
Eric Dalton Approach "treat bones like soft tissues"
те нажимаем на кость на место прикрепления мышцы.
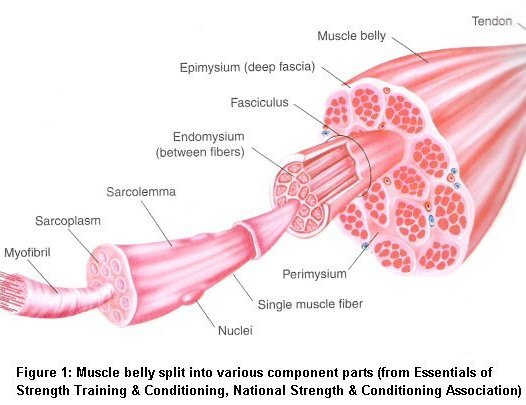
Muscle Fibers inserts into Fascia-> Fascia make tendon* -> Tendon Inserts Into Periostenum
Periostenum - покрывает кости, густо инервирован
Работая с костью как с софт tissue воздействуем на mechanoresoptors в periostenum: rufini, picinian corpusculs, intertetial, goldgi ogran
*tendon это как пучок фасциальных продолжений muscle fibers
воскресенье, 3 июля 2011 г.
пятница, 1 июля 2011 г.

среда, 29 июня 2011 г.
понедельник, 20 июня 2011 г.
Васильева, Л. Ф. «Визуальная диагностика нарушений статики и динамики опорно-двигательного аппарата человека»
Визуальная диагностика нарушений статики и динамики опорно-двигательного аппарата человека"
четверг, 16 июня 2011 г.
Abs reflect Low back
пятница, 10 июня 2011 г.
четверг, 9 июня 2011 г.
Muscle Tightness. From weakness or from restriction?
На деле это подтверждается тестами weak muscle в его short range и long range tight muscle.
Обычно tremor при muscle testing считают результатом weakness.
Я хотелбы сделать два предположения.
1. Мuscle pain, tr points, protective spasm is result from restriction that not allow proper functioning. Ex. Pain in LevatorScap, Supraspinatus <= tight infraspinatus
2.Тремор может быть также когда restriction не позволяет продолжить движение
мышца начинает получать прерывистиые сигналы от мозга что на другом конце (антагонист) срабатывает стретч рефлекс. Происходит постоянный interference from antagonist stretch reflex это нарушает neurological input и не дает мышце дальше сокращаться
3. Weakness может быть следствием overuse from restriction from antagonist
воскресенье, 29 мая 2011 г.
понедельник, 16 мая 2011 г.
суббота, 14 мая 2011 г.

четверг, 5 мая 2011 г.
YouTube - Muscle energy technique for posterior sacroiliac ligamant
пятница, 29 апреля 2011 г.
суббота, 23 апреля 2011 г.
пятница, 22 апреля 2011 г.
воскресенье, 17 апреля 2011 г.
Soft Tissue Manipulation and Pelvic Pain
Bialowsky (2009) reports that the effects of soft-tissue-focused manual therapies includes:
- Changes of blood levels of b-endorphin serotonin (Degenhardt et al 2007)
- Endogenous cannabinoids (McPartland et al 2005)
- Improved circulation and drainage
- Decreased muscle spasm
- Relaxation
- Re-alignment of soft tissues
- Breaking of adhesions
- Increased range of motion
- Removal of cellular exudates
Manual Therapy Approaches
The listing below of a selection of currently utilised manual therapy approaches that address fascial and myofascial dysfunction takes for granted that there would be simultaneous or subsequent focus on etiological features. Also, the seven modalities listed should not be regarded as definitive, as there are many other variations. However, those listed (and briefly discussed) represent a variety of validated biomechanical approaches, some of them novel and others well established.
- Connective tissue manipulation (ctm), as practised in relation to chronic pelvic pain, is a variation on the work of Dicke (1953) and Ebner (1975). Known in Germany where it was developed as "Bindegewebsmassage", it involves direct manual strokes, or forms of vigorous skin rolling, focused on connective tissue. Connective tissue is treated/mobilized until there is: improvement in mobility, decrease in sensitivity, and increase in warmth. Goals include: improved circulation; improved tissue integrity; decreased ischemia; reduced nocigenic chemicals in restricted connective tissue; decrease or elimination of visceral pain or dysfunction---possibly involving reflex effects; decrease in adverse neural tension on peripheral nerve branches.
- Fascial manipulation (FM). The key premise of FM is that fascia presents a specific organization and relationship with the underlying muscles. In particular, the fascia is seen as: coordinating element for motor units (grouped together in myofascial units); uniting element between unidirectional myofascial units (myofascial sequences); connecting element between body joints via myofascial expansions and retinacula (myofascial spirals). This model is supported by in-depth studies of fascial anatomy and physiology. Numerous dissections of unembalmed human cadavers have evidenced: muscular fibre insertions directly onto deep fascia (Stecco et al 2007); fibre distribution according to precise motor directions (Stecco et al 2008, 2009); myotendinous expansions that link adjacent segments (Stecco et al 2009). Extensive histological analysis of deep muscular fascia has also provided evidence for hypotheses concerning fascia's role in proprioception and tensional force distribution within the fascial system. (Stecco et al 2006, 2007)
- Muscle Energy Technique defined as "a form of osteopathic manipulative diagnosis and treatment in which the patient's muscles are actively used on request, from a precisely controlled position, in a specific direction, and against a distinctly executed physician counterforce". (ECOP 2009) Various studies have demonstrated that muscle energy techniques increase muscle extensibility (Ballantyne et al 2003) and range of motion (Burns & Wells 2006) including thoracic rotation. (Lenehan et al 2003)
- Myofascial release. King (2010) notes that myofascial release (MFR) is "a system of diagnosis and treatment first described by AT Still, and his early students, which involves continual palpatory feedback to achieve release of myofascial tissues."
Direct MFR: A myofascial tissue restrictive barrier is engaged for the myofascial tissues and the tissue is loaded with constant force, until tissue release occurs.
Indirect MFR: The dysfunctional tissues are guided along the path of least resistance, until free movement is achieved. (ECOP 2009) - Scar tissue release. Kobesova et al (2007) suggest that scars may develop adhesive properties that compromise tissue tensioning, altering proprioceptive input, behaving in much the same way as active myofascial trigger points. It is suggested that faulty afferent input can result in disturbed efferent output leading to (for example): protective postural patterns, increased neurovascular activity, and pain syndromes. The term active scar is designated to describe the ongoing additional neural activity associated with adhesive scar formations.
- Straincounterstrain (SCS). Osteopathic system of diagnosis and indirect treatment, in which the patient's somatic dysfunction is treated, using passive positioning, resulting in spontaneous tissue release. (ECOP 2009) SCS technique involves shortening myofascial structures to reduce the nociceptive experience arising from firm palpation of a tenderpoint in the dysfunctional tissues.
- Trigger point deactivation methods. Montenegro et al (2009) insist that myofascial pain syndrome should always be considered as part of the differential diagnosis of chronic pelvic pain. Systematic reviews have investigated the effectiveness of soft tissue manual intervention for inactivating trigger points (TrPs) (Fernandez-de-las-Penas et al 2005, Rickards 2006, Vernon & Schneider 2009). Anderson et al (2009) have identified the most common location of TrPs related to pelvic pain: pubococcygeus (90%), external oblique (80%), rectus abdominis (75%), hip adductors (19%), gluteus medius (18%).
These themes are explored further on my blog http://chaitowschat-leon.blogspot.com/ and Web site www.leonchaitow.com/index.htm.
To Study
http://www.stretchingusa.com
2) Orthopedic Massage with James Waslaski
http://www.healingartsinstitute.com/shop/category.asp?catid=370
http://www.orthomassage.net/
3)Resistance Release Training with Deane Juhan
http://www.jobsbody.com/
Combination
PNF->AIS->Orthopedic Massage
Iliotibial Band Treatment
Some therapists work directly on the IT band, but because it is a long tendon it does not stretch. A much better way of lengthening the IT band is to stretch the muscles that attach into this long tendon, which are the tensor fascia lata and the lateral fibers of the gluteus maximus.
This 22 minute video shows a treatment of a client with a knee replacement and a tight iliotibial band. Rather than focusing only on the problem area, the therapist does an assessment and treatment of all the related structures, using techniques from a number of different modalities. Techniques used include PNF Stretching, Reciprocal Inhibition, Active Isolated Stretching, and lengthening of muscles while using eccentric contraction.
The therapist, Mike Sweet, is a graduate of Healing Arts Institute. He has taken many advanced classes, including Orthopedic Massage with James Waslaski, and Resistance Release Training with Deane Juhan.
Pain Caused By Low Back Ligaments


Check Humstring by Resisted Test.
Pain in calf cause only Sac.Tub.Lig.
Do Palpation Test.
Usualy Trauma in Lateral Margin of the Sacrum.
YouTube - Muscle energy technique for posterior sacroiliac ligamant
Right on left sacral torsion - Muscle Energy Technique (M1) by Tom Ockler
Muscle Energy Seminars and Courses
Video Excerpts from the M1 Course
Ortho-Bionomy by Jim Berns
Ortho-Bionomy was developed by a British doctor, Arthur Lincoln Pauls, in his early years as an Osteopath. Before practicing Osteopathy Dr. Pauls was a Judo instructor. Every day in Judo he practiced the principle of following someone's movement and energy in the direction they were going, and if possible exaggerating that direction. Yet when Arthur went to Osteopathy school and learned all the medical and manipulative techniques at that time, he was disturbed to find that his teachers did not understand this principle.
When I was first introduced to Ortho-Bionomy, I had been doing massage therapy for a few years and was close to being burned out. I had studied (and was quite good at) a wide variety of therapies from deep-tissue to subtle energy work. But there was a part of me that was frustrated with the chronic reoccurrence of the same problems.Clients would come in with certain muscle contractions; I would stretch them out and then they would come back a week or two later with the same patterns. I was worn out by the struggle of fighting their body: trying to move it from where it was to where I thought it should be. Inside of me somewhere, I believed there must be an easier way to help people out of their pain.
суббота, 16 апреля 2011 г.
To review. Ilio-Sacral Diagnosis and Treatment, Part Three: Gluteus Medius, Piriformis and Pubic Symphysis - Positional Release and Rehabilitation Exercises
Довольно интересная статья
Counterstrain for Gluteus Medius

"Classic counterstrain requires you to hold this position for 90 seconds. (Yes, 90 seconds seems like forever, and some say you can shorten the time to 20 to 30 seconds by doing a brief, gentle contract-relax of the muscle involved or its antagonist.[???тут вот мне не совсем понятно надо подумать???]) When you are done, slowly let the leg back down. Don't let the patient help you; come out of the position with the patient as passive as possible. Retest with pressure on the tender point. When you are done, if the technique was correct, there will be a dramatic diminishing of the tenderness."
В очередной раз говорится о важности укрепления gluteus medius для стабилизации pelvis, обычно ослаблены

как я понимаю если поднимать сильнее будут включаться
transverse obliqu, quadratus lumborum
живот втянуть, стопа параллельно полу
Также рекомендуется растягивать periformis, он обычно tight & short

Shears - это upslip downslip
Flares - это открытый закрытый полутаз (inflare outflare)
Subluxation | Qualities | Keys |
shears upslip/downslip | all landmarks are inferior or superior; stiff side resists inferior or superior motion | assess both supine and prone nonphysiological shear |
flares internal/external | ASIS stuck medial or lateral | tender medial side of ASIS |
sagittal rotation PI and AS | usually a compensation; ASIS inferior or superior | don't correct over and over |
ilio-sacral separation | ilium resists medial motion; can coexist with hypermobility of same side | check gluteus medius |
pubic symphysis | separation and inferior/superior | tender lateral border of tubercles |
Примечательно что автор счтитает rotation in sa
THE BOOK. Positional Release Therapy
| Positional Release Therapy -- Assessment and Treatment of Musculoskeletal Dysfunction | |
| Kerry J. D'Ambrogio, PT, George B. Roth, DC, ND Very good book about strain counterstrain. Excelent pictures. Discussion about effects & mechanic of CS. |
пятница, 15 апреля 2011 г.

Low Force MethodologyBy Marc Heller, DC |
The Books TO READ
*****1) Fascial manipulation for muscuskeletal pain By Luigi Stecco //the best book about facsia
Fascia coordinate movements. Important role in movements. Motion unit. Control Point in Motor unit.
New approach for reabilitation. Parallel with meridians Tr.Points etc.
Good for practitioner who suffer from mf pain
2) Anatomy trains: myofascial meridians for manual and movement therapists
3)
Trigger Points and Muscle Chains in Osteopathy
By Philipp Richter, Eric Hebgen*****4) Myofascial Chains by Leopold Busquet //не знаю точно названия
среда, 6 апреля 2011 г.



понедельник, 4 апреля 2011 г.
Proprioreseptive Input. Activation exercises
It is important to note that when performing concentric contractions alone, there may be a resultant unloading of the muscle spindle and decreased facilitation from the stretch reflexes as the muscle moves into the shortened range. Therefore, concentric contractions are ineffective and even detrimental when attempting to improve proprioceptive input to an inhibited muscle. [from MAT description]What is Proorioreceotive Input(PI).
Why Spindels have less PI in shortened position?
What is Activation Exercise?
How to do Activation Exercise?
http://www.coachr.org/ankleproprio.htm
http://www.muscleactivation.com/FAQ.html
воскресенье, 3 апреля 2011 г.
Kinesiology

Lecture Topics in Kinesiology
(from course materials developed for the Department of Rehabilitation Science, 1988-2001)
http://moon.ouhsc.edu/dthompso/namics/lecsked.htm
Effects of chronic lengthening or shortening of muscle: "stretch weakness" and "adaptive shortening" http://moon.ouhsc.edu/dthompso/namics/immob.htm
Length-associated (mechanical) properties of muscle http://moon.ouhsc.edu/dthompso/namics/actpass.htm
суббота, 2 апреля 2011 г.
CROSS FIBER FRICTION TECHNIQUES
|

пятница, 1 апреля 2011 г.
Graston Technique
Joing Instability =>Guarding =>Tightness (Fascial & Muscle Fibrosis)
No Strengthen + Soft Tissue Mobilization => No Stability & Worsen Condition
balance mobility/stability
Shift from Dynamic Stability (muscles) to Static Stability (fibrous tissues)
Наращивание соединительной фиброзной ткани - процесс защиты и старения
Tight Fascia + muscle contracted => constrict muscle belly / unable to fully contract, ischemia, decreased circulation
Gluteus Medius Tendenitis
тут же напрягается QL тк Hip Bone goes to Abduction + Posterior-External Rotation.
Psoas тоже напрягается так как Hip Bone идет в Posterior Rotation Psoas work eccentrically чтобы удержать осанку прямое положение спины.
При этом атрофируется Pectineus тк при данном движении Hip Bone уменьшается длинна покоя те уменьшается расстояние между точками прикрепления Pectineus. В результате происходит immobilization in short range / on slack=> атрофия
После часа сидения возникла постоянная боль. По всей площади бедра отдает в пах.
четверг, 31 марта 2011 г.


среда, 30 марта 2011 г.
Integral Bodywork Approach
1) Counter Strain. Problems: Tender points, Tr.Points. Purpose: Local Proprioreceptive Relaxation.
2) Ortho-Binomica [Osteopatic] Purpose: Global Proprioreceptive Relaxation
SOFT TISSUE WORK
3) Warm up. Purpose: Prepare Soft for further work.
a)Hit:{Hot Pack; Hot Stones}
b) Superficial Massage: Techniques: Eflorage, Petrisage, Kneading
(поглаживание, разминание, выжимание) Time: 1-3 min. Superficial massage. speed start from Medium increase temp to fast.
4)
вторник, 29 марта 2011 г.
Use of Hip External and Internal Rotators in Preventing Spine Related Injuries
External Rotators Internal Rotators
Psoas Major Gluteus minimus
Iliacus Gluteus Medius (anterior)
Sartorius Tensor fasciae latae
Gluteus Maximus Adductor longus
Piriformis Semimembranosus
Quadratus femoris Semitendinosus
Gemellus superior and inferior
Obturator externus and internus
Gluteus medius (posterior)
As mentioned in the above text, lumbo pelvic posture may be affected with tight and/or weak hip
rotators. If the athlete/client experiences tight hip external rotators, pelvic positioning may be altered.
This tightness may cause the pelvis to retrovert (posterior tilt) due to the insertion into sacrum, and the
thoracolumbar fascia, which may further affect the positioning of the lumbar spine. Due to this
posterior pelvic tilt, the lumbar spine takes on a flexed disposition, which is commonly referred to as“flat back”. This affects the curvature of the lumbar spine (flattens back and decreases lordotic
curvature of the lumbar spine). This postural distortion may place unwanted stress to the low back and
cause future trauma to the lumbar region. This may be the cause of bulging and/or herniated disks
(Regan, 2000).
In contrast, tight hip internal rotators may cause an anteverted pelvis (anteriorly tilted pelvis), which
increases the lordotic curvature of the spine placing stress on this area. Injuries may occur to athletes
via stress to the pars interarticularis and facet joints (Regan, 2000). Both of these compensatory factors
affect the integrity of the lumbar spine. Tight hip rotators may pose to be problematic to athletes in
sports such as hockey, tennis and auto racing. When the hip rotators are tight, the athlete many times
compensates with rotation of the lumbar spine. The lumbar spine is composed of five vertebrae which
increase is size superior to inferior. This area is built more for stability versus mobility as excessive
rotation to this area may cause injury during athletic performance. Please view Table 2.0 for a look at
the healthy spine.
Having strong, flexible hip rotators can allow for optimum performance and decrease the
strain/pressure placed on other regions of the body (lumbar spine, thoracic spine, and SI joint). This
will allow movement patterns to occur more efficiently increasing performance standards and ensuring
the integrity of the athletes’ health in regards to preventing sports related injury.
References:
(1) Boyle, Michael, Functional Training For Sports, Human Kinetics, Copyright 2004, pp. 85-91.
(2) Frederic, D, Strength Training Anatomy, Human Kinetics, Copyright 2001, pp. 71- 74.
(3) Ninos, J, A Chain Reaction: The Hip Rotators, Strength and Conditioning Journal, 2001, Vol. 23,
No.2, pp. 26-27.(4) Regan, D, Implications of Hip Rotators in Lumbar Spine Injuries, Strength and Conditioning
Journal, December 2000, Vol.22, No.6, pp. 7-13.
понедельник, 28 марта 2011 г.



Adductor Strain. Iliopsoas Tendinitis. Research
http://emedicine.medscape.com/article/307308-overview
Physical
- Iliopsoas strain - Hip flexion against resistance is painful. Tenderness is difficult to localize because the insertion of the iliopsoas is deep.
- Osteitis pubis - Tenderness of the symphysis pubis and possible loss of full rotation of one or both hip joints are noted.
- Conjoined tendon lesions (ie, sportsman's hernia) - Exquisite tenderness upon palpation at the inguinal canal. Having the patient cough reproduces pain.
- Obturator neuropathy - Adductor muscle weakness, muscle spasm, and paresthesia over the medial aspect of the distal thigh may be present. Loss of adductor tendon reflex with preservation of other muscle stretch reflexes often is observed. A positive Howship-Romberg sign (medial knee pain induced by forced hip abduction, extension, and internal rotation) sometimes is observed.
ILIOPSOAS TENDINITIS
http://emedicine.medscape.com/article/90993-overview
Physical
- Inspection
- The hip may be held in slight flexion and external rotation to ease tension on the musculotendinous unit.
- Gait may demonstrate a shortened stride length on the affected side and increased knee flexion in the heel strike and midstance phases.
- Palpation
- An anterior pelvic tilt may be appreciated due to subsequent tightening of the iliopsoas muscle.//при posterior pelvic tilt мы полагаем weak-tender iliacus ?????
- Direct deep palpation to the area of the femoral triangle, which is bordered superiorly by the ilioinguinal ligament, medially by the adductor longus muscle, and laterally by the sartorius muscle, results in direct palpation of the iliopsoas musculotendinous junction.
- Tenderness over the iliopsoas tendon's insertion may be noted by palpating the lesser trochanter under the gluteal fold with the patient lying in a prone position.
- Functional testing
- Functional testing includes resisted hip flexion at 15° with palpation of the psoas muscle below the lateral half of the inguinal ligament.
- The patient also may be asked to sit with knees extended and subsequent elevation of the heel on the affected side. Pain caused by this maneuver (a positive Ludloff sign) is consistent with an iliopsoas tendinitis because the iliopsoas is the sole hip flexor activated in this position.
- The snapping(щелчок) hip sign or extension test also may be performed. Start with the affected hip in a flexed, abducted, and externally rotated position ????(knee is flexed for ease of testing), and passively move the hip into extension.???? This may result in an audible snap or palpable impulse over the inguinal region. Pain associated with this maneuver is highly suggestive of iliopsoas tendinitis or bursitis.
Femoral Triangle - bordered superiorly by the ilioinguinal ligament, medially by the adductor longus muscle, and laterally by the sartorius muscle

-----------------------------
SNAPPING HIP SINDROME -snapping (щелчок) sensation when hip flexed or extended.
Extra-articular
- Lateral extra articular
- Medial extra-articular
WHAT Test for Snapping Hip Syndrom ?
Pectineus. By its external border with the psoas. // поэтому при его дисфункции будет страдать и psoas