ADDUCTOR STRAIN
http://emedicine.medscape.com/article/307308-overview
ILIOPSOAS TENDINITIS
http://emedicine.medscape.com/article/90993-overview
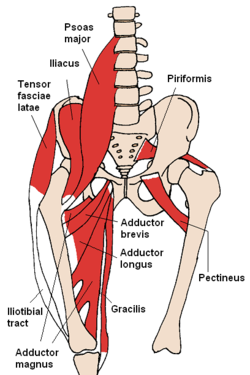
Femoral Triangle - bordered superiorly by the ilioinguinal ligament, medially by the adductor longus muscle, and laterally by the sartorius muscle

-----------------------------
SNAPPING HIP SINDROME -snapping (щелчок) sensation when hip flexed or extended.
WHAT Test for Snapping Hip Syndrom ?
Pectineus. By its external border with the psoas. // поэтому при его дисфункции будет страдать и psoas

http://emedicine.medscape.com/article/307308-overview
Physical
The acute adductor strain commonly occurs at the musculotendinous junction.
Tenderness, swelling, and ecchymosis can be observed at the superior medial thigh. Sometimes, a defect in the muscle can be palpated.
Pain is noted with resisted adduction and full passive abduction of the hip.
A pure hip adductor strain can be distinguished from combination injuries involving the hip flexors (ie, iliopsoas, rectus femoris) by having the patient lie in the supine position. If more discomfort is reproduced with resistive adduction when the knee and hip are extended than if the hip and knee are flexed, a pure hip adductor strain can be assumed.
Physical findings can help distinguish adductor strains from other causes of groin pain such as the following:
- Iliopsoas strain - Hip flexion against resistance is painful. Tenderness is difficult to localize because the insertion of the iliopsoas is deep.
- Osteitis pubis - Tenderness of the symphysis pubis and possible loss of full rotation of one or both hip joints are noted.
- Conjoined tendon lesions (ie, sportsman's hernia) - Exquisite tenderness upon palpation at the inguinal canal. Having the patient cough reproduces pain.
- Obturator neuropathy - Adductor muscle weakness, muscle spasm, and paresthesia over the medial aspect of the distal thigh may be present. Loss of adductor tendon reflex with preservation of other muscle stretch reflexes often is observed. A positive Howship-Romberg sign (medial knee pain induced by forced hip abduction, extension, and internal rotation) sometimes is observed.
ILIOPSOAS TENDINITIS
http://emedicine.medscape.com/article/90993-overview
Physical
Physical examination should focus on complete examination of the abdomen, hip, and groin. In females, a complete pelvic examination also should be considered.
- Inspection
- The hip may be held in slight flexion and external rotation to ease tension on the musculotendinous unit.
- Gait may demonstrate a shortened stride length on the affected side and increased knee flexion in the heel strike and midstance phases.
- Palpation
- An anterior pelvic tilt may be appreciated due to subsequent tightening of the iliopsoas muscle.//при posterior pelvic tilt мы полагаем weak-tender iliacus ?????
- Direct deep palpation to the area of the femoral triangle, which is bordered superiorly by the ilioinguinal ligament, medially by the adductor longus muscle, and laterally by the sartorius muscle, results in direct palpation of the iliopsoas musculotendinous junction.
- Tenderness over the iliopsoas tendon's insertion may be noted by palpating the lesser trochanter under the gluteal fold with the patient lying in a prone position.
- Functional testing
- Functional testing includes resisted hip flexion at 15° with palpation of the psoas muscle below the lateral half of the inguinal ligament.
- The patient also may be asked to sit with knees extended and subsequent elevation of the heel on the affected side. Pain caused by this maneuver (a positive Ludloff sign) is consistent with an iliopsoas tendinitis because the iliopsoas is the sole hip flexor activated in this position.
- The snapping(щелчок) hip sign or extension test also may be performed. Start with the affected hip in a flexed, abducted, and externally rotated position ????(knee is flexed for ease of testing), and passively move the hip into extension.???? This may result in an audible snap or palpable impulse over the inguinal region. Pain associated with this maneuver is highly suggestive of iliopsoas tendinitis or bursitis.
Femoral Triangle - bordered superiorly by the ilioinguinal ligament, medially by the adductor longus muscle, and laterally by the sartorius muscle

-----------------------------
SNAPPING HIP SINDROME -snapping (щелчок) sensation when hip flexed or extended.
Extra-articular
- Lateral extra articular
The more common lateral extra articular type of snapping hip syndrome occurs when the iliotibial band, tensor fascia lata, or gluteus medius tendon slides back and forth across thegreater trochanter. This normal action becomes a snapping hip syndrome when one of these connective tissue bands thickens and catches with motion. The underlying bursa may also become inflamed, causing a painful external snapping hip syndrome.
- Medial extra-articular
Less commonly, the iliopsoas tendon catches on the anterior inferior iliac spine (AIIS), the lesser trochanter, or the iliopectineal ridge during hip extension, as the tendon moves from an anterior lateral (front, side) to a posterior medial (back, middle) position. With overuse, the resultant friction may eventually cause painful symptoms, resulting in muscle trauma, bursitis, or inflammation in the area.
WHAT Test for Snapping Hip Syndrom ?
Pectineus. By its external border with the psoas. // поэтому при его дисфункции будет страдать и psoas
It is one of the muscles primarily responsible for hip flexion. It also adducts and medially(internaly) rotates the thigh. The pectineus muscle is the most anterior adductor of the hip.
Conclution: Pectineus выполняет Hip Flexion+Adduction+Internal Rot. Assist Psoas (one kinetic chain)
Делает приведение Hip & приведение Hip Bone. WHY? <={ origin from pubis insertion femur=>
приводит Femur (internal rotation). Femur в отведеном положении (slight external rotation) => Iliasus растягивается => тянет Hip Bone в Adduction (отведение) }
Pectineus Weak-Long => Femur Ext Rotation => Iliapsoas Stress ->Tightness => Hip Bone Abduction (раскрытие) => SIAI(anterior inferior)-Femur Impingement Syndrom in Hip Flexion (Knee Flexed) Adduction Internal Rotation
Комментариев нет:
Отправить комментарий