четверг, 31 марта 2011 г.


среда, 30 марта 2011 г.
Integral Bodywork Approach
NEUROGICAL RELAXATION
1) Counter Strain. Problems: Tender points, Tr.Points. Purpose: Local Proprioreceptive Relaxation.
2) Ortho-Binomica [Osteopatic] Purpose: Global Proprioreceptive Relaxation
SOFT TISSUE WORK
3) Warm up. Purpose: Prepare Soft for further work.
a)Hit:{Hot Pack; Hot Stones}
b) Superficial Massage: Techniques: Eflorage, Petrisage, Kneading
(поглаживание, разминание, выжимание) Time: 1-3 min. Superficial massage. speed start from Medium increase temp to fast.
4)
1) Counter Strain. Problems: Tender points, Tr.Points. Purpose: Local Proprioreceptive Relaxation.
2) Ortho-Binomica [Osteopatic] Purpose: Global Proprioreceptive Relaxation
SOFT TISSUE WORK
3) Warm up. Purpose: Prepare Soft for further work.
a)Hit:{Hot Pack; Hot Stones}
b) Superficial Massage: Techniques: Eflorage, Petrisage, Kneading
(поглаживание, разминание, выжимание) Time: 1-3 min. Superficial massage. speed start from Medium increase temp to fast.
4)
вторник, 29 марта 2011 г.
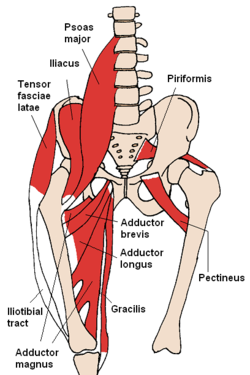
Use of Hip External and Internal Rotators in Preventing Spine Related Injuries
http://www.donskovsc.com/articles/fiofthep.pdf
External Rotators Internal Rotators
Psoas Major Gluteus minimus
Iliacus Gluteus Medius (anterior)
Sartorius Tensor fasciae latae
Gluteus Maximus Adductor longus
Piriformis Semimembranosus
Quadratus femoris Semitendinosus
Gemellus superior and inferior
Obturator externus and internus
Gluteus medius (posterior)
As mentioned in the above text, lumbo pelvic posture may be affected with tight and/or weak hip
rotators. If the athlete/client experiences tight hip external rotators, pelvic positioning may be altered.
This tightness may cause the pelvis to retrovert (posterior tilt) due to the insertion into sacrum, and the
thoracolumbar fascia, which may further affect the positioning of the lumbar spine. Due to this
posterior pelvic tilt, the lumbar spine takes on a flexed disposition, which is commonly referred to as“flat back”. This affects the curvature of the lumbar spine (flattens back and decreases lordotic
curvature of the lumbar spine). This postural distortion may place unwanted stress to the low back and
cause future trauma to the lumbar region. This may be the cause of bulging and/or herniated disks
(Regan, 2000).
In contrast, tight hip internal rotators may cause an anteverted pelvis (anteriorly tilted pelvis), which
increases the lordotic curvature of the spine placing stress on this area. Injuries may occur to athletes
via stress to the pars interarticularis and facet joints (Regan, 2000). Both of these compensatory factors
affect the integrity of the lumbar spine. Tight hip rotators may pose to be problematic to athletes in
sports such as hockey, tennis and auto racing. When the hip rotators are tight, the athlete many times
compensates with rotation of the lumbar spine. The lumbar spine is composed of five vertebrae which
increase is size superior to inferior. This area is built more for stability versus mobility as excessive
rotation to this area may cause injury during athletic performance. Please view Table 2.0 for a look at
the healthy spine.
Having strong, flexible hip rotators can allow for optimum performance and decrease the
strain/pressure placed on other regions of the body (lumbar spine, thoracic spine, and SI joint). This
will allow movement patterns to occur more efficiently increasing performance standards and ensuring
the integrity of the athletes’ health in regards to preventing sports related injury.
References:
(1) Boyle, Michael, Functional Training For Sports, Human Kinetics, Copyright 2004, pp. 85-91.
(2) Frederic, D, Strength Training Anatomy, Human Kinetics, Copyright 2001, pp. 71- 74.
(3) Ninos, J, A Chain Reaction: The Hip Rotators, Strength and Conditioning Journal, 2001, Vol. 23,
No.2, pp. 26-27.(4) Regan, D, Implications of Hip Rotators in Lumbar Spine Injuries, Strength and Conditioning
Journal, December 2000, Vol.22, No.6, pp. 7-13.
External Rotators Internal Rotators
Psoas Major Gluteus minimus
Iliacus Gluteus Medius (anterior)
Sartorius Tensor fasciae latae
Gluteus Maximus Adductor longus
Piriformis Semimembranosus
Quadratus femoris Semitendinosus
Gemellus superior and inferior
Obturator externus and internus
Gluteus medius (posterior)
As mentioned in the above text, lumbo pelvic posture may be affected with tight and/or weak hip
rotators. If the athlete/client experiences tight hip external rotators, pelvic positioning may be altered.
This tightness may cause the pelvis to retrovert (posterior tilt) due to the insertion into sacrum, and the
thoracolumbar fascia, which may further affect the positioning of the lumbar spine. Due to this
posterior pelvic tilt, the lumbar spine takes on a flexed disposition, which is commonly referred to as“flat back”. This affects the curvature of the lumbar spine (flattens back and decreases lordotic
curvature of the lumbar spine). This postural distortion may place unwanted stress to the low back and
cause future trauma to the lumbar region. This may be the cause of bulging and/or herniated disks
(Regan, 2000).
In contrast, tight hip internal rotators may cause an anteverted pelvis (anteriorly tilted pelvis), which
increases the lordotic curvature of the spine placing stress on this area. Injuries may occur to athletes
via stress to the pars interarticularis and facet joints (Regan, 2000). Both of these compensatory factors
affect the integrity of the lumbar spine. Tight hip rotators may pose to be problematic to athletes in
sports such as hockey, tennis and auto racing. When the hip rotators are tight, the athlete many times
compensates with rotation of the lumbar spine. The lumbar spine is composed of five vertebrae which
increase is size superior to inferior. This area is built more for stability versus mobility as excessive
rotation to this area may cause injury during athletic performance. Please view Table 2.0 for a look at
the healthy spine.
Having strong, flexible hip rotators can allow for optimum performance and decrease the
strain/pressure placed on other regions of the body (lumbar spine, thoracic spine, and SI joint). This
will allow movement patterns to occur more efficiently increasing performance standards and ensuring
the integrity of the athletes’ health in regards to preventing sports related injury.
References:
(1) Boyle, Michael, Functional Training For Sports, Human Kinetics, Copyright 2004, pp. 85-91.
(2) Frederic, D, Strength Training Anatomy, Human Kinetics, Copyright 2001, pp. 71- 74.
(3) Ninos, J, A Chain Reaction: The Hip Rotators, Strength and Conditioning Journal, 2001, Vol. 23,
No.2, pp. 26-27.(4) Regan, D, Implications of Hip Rotators in Lumbar Spine Injuries, Strength and Conditioning
Journal, December 2000, Vol.22, No.6, pp. 7-13.
понедельник, 28 марта 2011 г.



Adductor Strain. Iliopsoas Tendinitis. Research
ADDUCTOR STRAIN
http://emedicine.medscape.com/article/307308-overview
ILIOPSOAS TENDINITIS
http://emedicine.medscape.com/article/90993-overview
Femoral Triangle - bordered superiorly by the ilioinguinal ligament, medially by the adductor longus muscle, and laterally by the sartorius muscle

-----------------------------
SNAPPING HIP SINDROME -snapping (щелчок) sensation when hip flexed or extended.
WHAT Test for Snapping Hip Syndrom ?
Pectineus. By its external border with the psoas. // поэтому при его дисфункции будет страдать и psoas

http://emedicine.medscape.com/article/307308-overview
Physical
The acute adductor strain commonly occurs at the musculotendinous junction.
Tenderness, swelling, and ecchymosis can be observed at the superior medial thigh. Sometimes, a defect in the muscle can be palpated.
Pain is noted with resisted adduction and full passive abduction of the hip.
A pure hip adductor strain can be distinguished from combination injuries involving the hip flexors (ie, iliopsoas, rectus femoris) by having the patient lie in the supine position. If more discomfort is reproduced with resistive adduction when the knee and hip are extended than if the hip and knee are flexed, a pure hip adductor strain can be assumed.
Physical findings can help distinguish adductor strains from other causes of groin pain such as the following:
- Iliopsoas strain - Hip flexion against resistance is painful. Tenderness is difficult to localize because the insertion of the iliopsoas is deep.
- Osteitis pubis - Tenderness of the symphysis pubis and possible loss of full rotation of one or both hip joints are noted.
- Conjoined tendon lesions (ie, sportsman's hernia) - Exquisite tenderness upon palpation at the inguinal canal. Having the patient cough reproduces pain.
- Obturator neuropathy - Adductor muscle weakness, muscle spasm, and paresthesia over the medial aspect of the distal thigh may be present. Loss of adductor tendon reflex with preservation of other muscle stretch reflexes often is observed. A positive Howship-Romberg sign (medial knee pain induced by forced hip abduction, extension, and internal rotation) sometimes is observed.
ILIOPSOAS TENDINITIS
http://emedicine.medscape.com/article/90993-overview
Physical
Physical examination should focus on complete examination of the abdomen, hip, and groin. In females, a complete pelvic examination also should be considered.
- Inspection
- The hip may be held in slight flexion and external rotation to ease tension on the musculotendinous unit.
- Gait may demonstrate a shortened stride length on the affected side and increased knee flexion in the heel strike and midstance phases.
- Palpation
- An anterior pelvic tilt may be appreciated due to subsequent tightening of the iliopsoas muscle.//при posterior pelvic tilt мы полагаем weak-tender iliacus ?????
- Direct deep palpation to the area of the femoral triangle, which is bordered superiorly by the ilioinguinal ligament, medially by the adductor longus muscle, and laterally by the sartorius muscle, results in direct palpation of the iliopsoas musculotendinous junction.
- Tenderness over the iliopsoas tendon's insertion may be noted by palpating the lesser trochanter under the gluteal fold with the patient lying in a prone position.
- Functional testing
- Functional testing includes resisted hip flexion at 15° with palpation of the psoas muscle below the lateral half of the inguinal ligament.
- The patient also may be asked to sit with knees extended and subsequent elevation of the heel on the affected side. Pain caused by this maneuver (a positive Ludloff sign) is consistent with an iliopsoas tendinitis because the iliopsoas is the sole hip flexor activated in this position.
- The snapping(щелчок) hip sign or extension test also may be performed. Start with the affected hip in a flexed, abducted, and externally rotated position ????(knee is flexed for ease of testing), and passively move the hip into extension.???? This may result in an audible snap or palpable impulse over the inguinal region. Pain associated with this maneuver is highly suggestive of iliopsoas tendinitis or bursitis.
Femoral Triangle - bordered superiorly by the ilioinguinal ligament, medially by the adductor longus muscle, and laterally by the sartorius muscle

-----------------------------
SNAPPING HIP SINDROME -snapping (щелчок) sensation when hip flexed or extended.
Extra-articular
- Lateral extra articular
The more common lateral extra articular type of snapping hip syndrome occurs when the iliotibial band, tensor fascia lata, or gluteus medius tendon slides back and forth across thegreater trochanter. This normal action becomes a snapping hip syndrome when one of these connective tissue bands thickens and catches with motion. The underlying bursa may also become inflamed, causing a painful external snapping hip syndrome.
- Medial extra-articular
Less commonly, the iliopsoas tendon catches on the anterior inferior iliac spine (AIIS), the lesser trochanter, or the iliopectineal ridge during hip extension, as the tendon moves from an anterior lateral (front, side) to a posterior medial (back, middle) position. With overuse, the resultant friction may eventually cause painful symptoms, resulting in muscle trauma, bursitis, or inflammation in the area.
WHAT Test for Snapping Hip Syndrom ?
Pectineus. By its external border with the psoas. // поэтому при его дисфункции будет страдать и psoas
It is one of the muscles primarily responsible for hip flexion. It also adducts and medially(internaly) rotates the thigh. The pectineus muscle is the most anterior adductor of the hip.
Conclution: Pectineus выполняет Hip Flexion+Adduction+Internal Rot. Assist Psoas (one kinetic chain)
Делает приведение Hip & приведение Hip Bone. WHY? <={ origin from pubis insertion femur=>
приводит Femur (internal rotation). Femur в отведеном положении (slight external rotation) => Iliasus растягивается => тянет Hip Bone в Adduction (отведение) }
Pectineus Weak-Long => Femur Ext Rotation => Iliapsoas Stress ->Tightness => Hip Bone Abduction (раскрытие) => SIAI(anterior inferior)-Femur Impingement Syndrom in Hip Flexion (Knee Flexed) Adduction Internal Rotation
Ilia Psoas rehab
Physical Therapy or Athletic Training Therapy and Rehabilitation
Both active and passive stretching exercises that include hip and knee extension should be the focus of the program. Stretching the hip into extension and limiting excessive knee flexionavoids placing the rectus femoris in a position of passive insufficiency, thereby maximizing the stretch to the iliopsoas tendon.[????????думаю это может значить что psoas надо растягивать когда с knee полусогнутой или выпрямленной] Strengthening exercises for the hip flexors may also be an appropriate component of the program. Education, a non-steroidal anti-inflammatory drug regimen, as well as activity modification or activity progression (or both) may be used. Once symptoms have decreased a maintenance program of stretching and strengthening can be initiated. Light aerobic activity (warmup) followed by stretching and strengthening of the properhamstring, hip flexors, and iliotibial band length is important for reducing recurrences.
Self-treatment
A self-treatment recommended by the U.S. Army for a soft tissue injury of the iliopsoas muscle treatment, like for other soft tissue injuries, is a HI-RICE (Hydration, Ibuprofen, Rest, Ice, Compression, Elevation) regimen lasting for at least 48 to 72 hours after the onset of pain. "Rest" includes such commonsense prescriptions as avoiding running or hiking (especially on hills), and avoiding exercises such as baseball, jumping, sit-ups or leg lifts/flutter kicks.
Stretching of the tight structures (piriformis, hip abductor, and hip flexor muscle) may alleviate the symptoms (see link, pg. 3, for examples) The involved muscle is stretched until the "feeling of stretch" fades away (from 45 seconds up to 3-4 minutes), repeated three times separated by 30 second to 1 minute rest periods, in sets performed three to four times daily for six to eight weeks.[6] This should allow the soldier to progress back into jogging until symptoms disappear.[6]
Active/Passive muscle Insufficiency
Principles of Medical Physiology
By Sabyasachi SircarActive & Passive Insufficiency [p 122]
Two joints muscles - cross two joints. Eg: Hamstrings, Rectus Femoris
Active Insufficiency - two joints muscle in excessively slack position. Eg. Difficulty in fingers flexion when wrist is flexed.
Passive Insufficiency - two joints muscle in excessively stretched position. Eg.
Hip extention + knee flexion => Hamstring in Active Insufficiency; Rectus Femoris in Passive Insufficiency
Hip Flexion + Knee Flexion => Hamstring in Passive Insufficiency; Rectus Femoris in Active Insufficiency
p.124
Skeletal Lever System
Class 1 Lever: Neck Extensors
Class 2 Lever: Masseter // few examples
Class 3 Lever: Bracialis // самый распространенный вариант

Physical Therapy Diagnosis: Lumbar Stabilization
The Main Idea.
Perform exercise with spine stabilization for strengthening Transverse Abs & Multifidius (core stabilisers).
Впринципе большинство упражнений рекомендуется делать с активацией core stabilisers.
Perform exercise with spine stabilization for strengthening Transverse Abs & Multifidius (core stabilisers).
Впринципе большинство упражнений рекомендуется делать с активацией core stabilisers.
четверг, 24 марта 2011 г.
C7 paravertebral muscles lengthening/shortening
paravertebral muscles/С7 area /Right side / lengthening action - F Sl Rl
shortening action - E Sr Rl

shortening action - E Sr Rl

среда, 23 марта 2011 г.
Great Physicians to know
- Janet Travell, MD
- David Simons, MD
- Geoffrey Maitland, PT
- David Butler, PT
- Leon Chaitow, DO
- Dr. Lawrence Jones
- Freddy Kaltenborn, PT
- Stanley V. Paris Ph.D., P.T.
- Robin McKenzie, PT
- Vladimir Janda, MD
- Karel Lewit, MD, & others.

Janda Approach
http://www.jandaapproach.com/about/
Muscle Imbalance, patterns, predictabel;
gluteus maximus - pelvic instability
ankle instability low back pain
http://www.jandaapproach.com/the-janda-approach/philosophy/
Muscle Imbalance, patterns, predictabel;
gluteus maximus - pelvic instability
ankle instability low back pain
http://www.jandaapproach.com/the-janda-approach/philosophy/
Structural vs Functional opproach
In musculoskeletal medicine, there are two main schools of thought, that is, a structural or functional approach. In the structural approach, the pathology of specific static structures is emphasized; this is the typical orthopaedic approach that emphasizes diagnosis based on localized evaluation and special tests (X-Ray, MRI, CT Scan, etc). On the other hand, the functional approach recognizes the function of all processes and systems within the body, rather than focusing on a single site of pathology. While the structural approach is necessary and valuable for acute injury or exacerbation, the functional approach is preferable when addressing chronic musculoskeletal pain.
A noxious stimulus is "an actually or potentially tissue damaging event.
Nociception (synonym: nocioception or nociperception) is defined as "the neural processes of encoding and processing noxious stimuli."[1] It is the afferent activity produced in the peripheral and central nervous system by stimuli that have the potential to damage tissue
-------------------------------------------------------------------------------------------------------------------------------------
sensorimotor system
Knee effusion
The Sensorimotor System
In chronic pain, special diagnostic tests of localized areas (for example, low back radiographs) are often normal, although the patient complains of pain. The site of pain is often not the cause of the pain. Recent evidence by supports the fact that chronic pain is centrally-mediated (Staud et al. 2001). Similarly, research on the efficacy of different modes of exercise management of chronic pain has shown a central effect of exercise in decreasing chronic low back pain (Mannion et al. 1999). This research supports the basis of Janda’s approach: the interdependence of the musculoskeletal and central nervous system. Janda states that these two anatomical systems cannot be separated functionally. Therefore, the term “sensorimotor” system is used to define the functional system of human movement. In addition, changes within one part of the system will be reflected by compensations or adaptations elsewhere within the system because of the body’s attempt at homeostasis (Panjabi, 1992).
Tonic and Phasic Muscle Systems
Janda identified two groups of muscles based on their phylogenetic development (Janda, 1987). Functionally, muscles can be classified as “tonic” or “phasic”. The tonic system consists of the “flexors”, and is phylogenetically older and dominant. These muscles are involved in repetitive or rhythmic activity (Umphred, 2001), and are activated in flexor synergies. The phasic system consists of the “extensors”, and emerges shortly after birth. These muscles work eccentrically against the force of gravity and emerge in extensor synergies (Umphred, 2001).
| Tonic Muscles Prone to Tightness or Shortness | Phasic MusclesProne to Weakness or Inhibition |
| Gastroc-SoleusTibialis Posterior Hip Adductors Hamstrings Rectus Femoris Iliopsoas Tensor Fascia Lata Piriformis Thoraco-lumbar extensors Quadratus Lumborum Pectoralis Major Upper Trapezius Levator Scapulae Scalenes Sternocleidomastoid Upper limb flexors | Peroneus Longus, BrevisTibialis Anterior Vastus Medialis, Lateralis Gluteus Maximus, Medius, Minimus Rectus Abdominus Serratus Anterior Rhomboids Lower Trapezius Deep neck flexors Upper limb extensors |
sensorimotor system
Knee effusion
суббота, 19 марта 2011 г.
Tenis Elbow Eccentric Strengthening Protocol
SUMMARY.
Treatment for Target muscles with Tendenitis/wrist extensors. Eccentric exercise. 1-3 lbs load.
Purpose: Strengthening & Elongating
Strengthening for opposite muscle group: Consentric
Purpose: Strengthening & Shortening
Using manually controlled resisting force through Thera-Band.
------------------------------------------------------------------------------------
http://totaltendon.com/
Treatment for Target muscles with Tendenitis/wrist extensors. Eccentric exercise. 1-3 lbs load.
Purpose: Strengthening & Elongating
Strengthening for opposite muscle group: Consentric
Purpose: Strengthening & Shortening
Using manually controlled resisting force through Thera-Band.
------------------------------------------------------------------------------------
http://totaltendon.com/
пятница, 18 марта 2011 г.
TFL != ITBand
{Adductors (straight leg) }Tight && {Hip Internal Rotators: TFL; Ant.Glut.Med} Weak =>
{ITBand} Tight/Shortened
{ITBand} Tight/Shortened
IliaPsoas Disfunction. Multifidus
Antagonism:
Psoas VS Multifidus
Iliacus VS Gluteus Max
Posture. Psoas/Multifidus.
Psoas moves spine down&forward
Multifidus moves up&back
Sinergism: Multifidus & Transverse obliques
Iliacus & Hip Internal Rotators // для поднимания бедра выше колена
{Gluteus Anterior;TFL} Weak => {Gluteus Medius Posterior} Tight => Adductors (knee flexed) weak
TFL weak => ITBand Tight
Psoas VS Multifidus
Iliacus VS Gluteus Max
Posture. Psoas/Multifidus.
Psoas moves spine down&forward
Multifidus moves up&back
Sinergism: Multifidus & Transverse obliques
Iliacus & Hip Internal Rotators // для поднимания бедра выше колена
{Gluteus Anterior;TFL} Weak => {Gluteus Medius Posterior} Tight => Adductors (knee flexed) weak
TFL weak => ITBand Tight
Adductors imbalance pattern
Tight Adductors => Weak Gluteus medius
Tight Adductors => Tight TFL
Adductors :
Stance leg stabilizer: Magnus
Longus Grasilis: Flexed 90 Leg Adduction
Brevis Pectineus: Assist Psoas with raising externaly rotated flexed leg
{Magnus Grasilis} Tight =>{Adductors Brevis Pectineus Longus }Weak
{Brevis Pectineus} => Iliacus Tight
{Ilia Psoas} Tight =>{Gluteus Max} Weak => {Hamstrings Magnus} Tight => {Glut.Med} Weak & {TFL Vast. Lat. } Tight
Tight Adductors => Tight TFL
Adductors :
Stance leg stabilizer: Magnus
Longus Grasilis: Flexed 90 Leg Adduction
Brevis Pectineus: Assist Psoas with raising externaly rotated flexed leg
{Magnus Grasilis} Tight =>{Adductors Brevis Pectineus Longus }Weak
{Brevis Pectineus} => Iliacus Tight
{Ilia Psoas} Tight =>{Gluteus Max} Weak => {Hamstrings Magnus} Tight => {Glut.Med} Weak & {TFL Vast. Lat. } Tight
Shoulder Stabilizers. Biceps Short Long Head
Biseps Triceps очень важны для стабилизации Humerouse Head в суставе.
Biceps Imbalance: Short Head usually weaker than long => Long Head Overuse=> Tendon Tear
Weak Supraspinatus => Levator scapula overuse //they attached to scapula adge have connected fascia
work as one chain
weak Deltoid => overuse of Supraspinatus
Biceps Long Head assist with arm raising + Weak Deltoid => Long Head overuse
Biceps Imbalance: Short Head usually weaker than long => Long Head Overuse=> Tendon Tear
Weak Supraspinatus => Levator scapula overuse //they attached to scapula adge have connected fascia
work as one chain
weak Deltoid => overuse of Supraspinatus
Biceps Long Head assist with arm raising + Weak Deltoid => Long Head overuse
Shoulder muscle imbalance pattern. Supraspinatus. Frozen shoulder
pullups (за голову )+ push-ups (широким хватом) = >Latisimus&Pectoralis tight=> external rotation restriction=>teres minor immobilization/weakness; rotator cuff overstres/tightness; weak upper Trap.=> sholder protraction&internal rotarion=> change length/load Supraspinatus=> ???Frozen shoulder???
P.S.
Сегодня испытал Frozen shoulder after prolong taping in standing position. Уверен это Supraspinatus
THE CYCLE OF SOMATIC DISFUNCTION. MUSCLE IMBALANCE
REASONS.
Overtrain/overload => (*) tightness Primary Actions Muscles
=>decrease ROM => immobilisation Secondary Action Muscle (eg rotators) => weakness => disability =>(*loop)=> tightness Primary Actions Muscles
------------------------------------------------
Primary Actions Muscles - phasic muscles, strong muscle with big force momentum have tendency to become tight from over
Secondary Action Muscles - phasic/tonic muscles assist in general movements eg rotators. Они короче обчыно имеют вращающий момент (крепятся дальше от оси вращения eg hip rotators, rotator cuff)
EXAMPLES: 1) Shoulder.
Primary - pectoralis, Latisimus;
Secondary - rotator cuff
2) Hip. Primary- Hamstring Quadriceps TFL Adductors; Gluteus Max; IlioPsoas
Secondary - Glut Med/Min Hip External Internal Rotators;
Overtrain-overload - перегрузка мышц too much repetitions/load. Вызывает боль, укорочение мышц
//----------------------------------------------
Dynamic:
Sudden overload ( Lifting);
Wrong movement (overcome physiological barrier);
Static overload(Prolonged position, bad posture)
Kinetic:
Tight Primary Action Muscles & Weakness Secondary Action Muscles ->
Changing in joint position;
Changing in Secondary Act.Muscles length/load ->
Constant Eccentric Load // postural muscles eg supraspinatus
Continues Concentric overload / // Hamstrings (weak glut.max);
Rectus femoris (weak psoas;
Immobilization (Locking in short range) -> ....
Overtrain/overload => (*) tightness Primary Actions Muscles
=>decrease ROM => immobilisation Secondary Action Muscle (eg rotators) => weakness => disability =>(*loop)=> tightness Primary Actions Muscles
RULE:
1. Disfunction usualy happens in Secondary Action Muscles OR Tonic-Postural muscles
2. If there is tightness in Primary Action Muscles => Look for disability/disfunction in Secondary Action Muscles
------------------------------------------------
Primary Actions Muscles - phasic muscles, strong muscle with big force momentum have tendency to become tight from over
Secondary Action Muscles - phasic/tonic muscles assist in general movements eg rotators. Они короче обчыно имеют вращающий момент (крепятся дальше от оси вращения eg hip rotators, rotator cuff)
EXAMPLES: 1) Shoulder.
Primary - pectoralis, Latisimus;
Secondary - rotator cuff
2) Hip. Primary- Hamstring Quadriceps TFL Adductors; Gluteus Max; IlioPsoas
Secondary - Glut Med/Min Hip External Internal Rotators;
Overtrain-overload - перегрузка мышц too much repetitions/load. Вызывает боль, укорочение мышц
//----------------------------------------------
Proper Stretch & Strengthening technique for Tr.Points
Proper Stretch Exercise technique for Tender/Tr Point muscles.
Stretch before pain barrier(No pain!!!). Hold for 5 sec. Every 1 hour. No discomfort or pain flare after stretching exercise.
Proper Strengthening Exercise Technique.
Adjust Repetition& weight so no paint increase after.
Twice a day. If feel pain increasing after decrease repetitions.
[http://musclespasmchainreaction.com]
Можно замораживать спреем и потом растягивать [Travell & Simons Trigger points munual]
как это понимать?
----------------------------------------------------------------------------------------?/
Stretch before pain barrier(No pain!!!). Hold for 5 sec. Every 1 hour. No discomfort or pain flare after stretching exercise.
Proper Strengthening Exercise Technique.
Adjust Repetition& weight so no paint increase after.
Twice a day. If feel pain increasing after decrease repetitions.
[http://musclespasmchainreaction.com]
Можно замораживать спреем и потом растягивать [Travell & Simons Trigger points munual]
/?---------------------------------------------------------------------------------------
Stretch exercise should also be done following trigger
point massage and following strengthening exercise.
как это понимать?
----------------------------------------------------------------------------------------?/
четверг, 17 марта 2011 г.
Forced stretch [osteopatic]
В теле есть сильные мышцы которые имеют тенденцию укорачиваться. Их надо постоянно растягивать. Например Hamstring, TFL, Rectus Femoris, Latisimus (sometimes).
Для таких мышц нужен стретч с весом или дополнительной нагрузкой или Assistance. Просто Active Stretch не достаточно.
Для таких мышц нужен стретч с весом или дополнительной нагрузкой или Assistance. Просто Active Stretch не достаточно.
среда, 16 марта 2011 г.
Short-Tight-Facilitating muscles
Overuse => Shortening -Tight - Overdevelopment => ROM restriction; Wrong byomechanic => Facilitation
Examples: TFL, Vastus Lateralis (facilitate Glut.Medi.), Hamstrings (facilitate Glut.Max.)
------------------------------------------------------------------
Facilitation - это когда мышца частично берет на себя функцию слабого агониста
Examples: TFL, Vastus Lateralis (facilitate Glut.Medi.), Hamstrings (facilitate Glut.Max.)
------------------------------------------------------------------
Facilitation - это когда мышца частично берет на себя функцию слабого агониста
Rotation - start point of disfunction
Muscles contraction Rule. Contracted muscle aim (стремиться) move origins & insertions to one plane
Joint Motion Rule: all movements in 3 planes
часто мышцы закручиваются вокруг кости => создают вращательный момент
Rule: attachment more far from axis => more moment of rotation. Чем дальше место прикрепления мышцы относительно оси вращения кости тем больше момент силы вращения. Те такие мышцы вероятнее вызовут вращение кости. Пример: Psoas. Attachment - lesser trochanter. Action - hip flexion with ext. rotation.
Muscle Shortening & Elongating
Shortening:
Repetitive rapid movements -> fatigue-> shortening
Isotonic Concentric exercise in Midle-Short Range.
Short ROM exercise in short range.
Isometric contraction in Shortened Position.
Eccentric Dynamic Momentum Stability Exercise in Middle Range
Elongating:
Isometric contraction in lengthened position
Isotonic Eccentric exercise in Migle-Long Range
Short ROM exercise in Long Range.
Repetitive rapid movements -> fatigue-> shortening
Isotonic Concentric exercise in Midle-Short Range.
Short ROM exercise in short range.
Isometric contraction in Shortened Position.
Eccentric Dynamic Momentum Stability Exercise in Middle Range
Elongating:
Isometric contraction in lengthened position
Isotonic Eccentric exercise in Migle-Long Range
Short ROM exercise in Long Range.
Васильева. Мышечный Суставной Связочный блок
Из семинара Дисфунции таза Васильевой.
мышечный блок => суставной => связочный
Treatment:
На каждом уровне каждая часть системы поддерживает данную дисфункцию данное
состояние. Чтобы эфективно лечить надо снять все три блока.
мышечный блок => суставной => связочный
Treatment:
На каждом уровне каждая часть системы поддерживает данную дисфункцию данное
состояние. Чтобы эфективно лечить надо снять все три блока.
Weakness. Inhabited. Tr.Points
TIGHT-SHORT-WEAK muscle.
Reasons?:
Neurological level - Inhibition
Hyperactive antagonist from other muscles
Nerve compression - low neurological input
Muscle block
Joints block
Somatic dysfunction
Functional Level - Weakness
Overuse -> Spastisity
Posture -> Contraction
Physical Stereotypes
Trauma - wrong movement
TR.POINTS
Is it from Weakness, Overuse, Chemical imbalance?
Weakness => Tr.Point OR Tr.Points =>Weakness + Stress ???
Tr.Points - maintain state of muscle disability (muscle block). Способствует сохранению блока в мышце
Reasons?:
Neurological level - Inhibition
Hyperactive antagonist from other muscles
Nerve compression - low neurological input
Muscle block
Joints block
Somatic dysfunction
Functional Level - Weakness
Overuse -> Spastisity
Posture -> Contraction
Physical Stereotypes
Trauma - wrong movement
TR.POINTS
Is it from Weakness, Overuse, Chemical imbalance?
Weakness => Tr.Point OR Tr.Points =>Weakness + Stress ???
Tr.Points - maintain state of muscle disability (muscle block). Способствует сохранению блока в мышце
Supraspinatus disfunction
Action: Инициирует поднятие руки, учавствуиет во всех движениях с поднятием руки. Фиксирует плечо в суставе.
Palpation: Руку на Scapula Spine. Поднятие руки 45 градусов между sagital & coronal planes. Почувтвуется лекое движение, натяжение под пальцем.
Учавствует во всех движениях с поднятием руки. Даже при болтании рукой при ходьбе. Держание портфеля в руке.

Reasons:
Dynamic: Wrong movenent: Поднятие тежестей, долгое держание руки на весу.
Kinetic: tight Pectoralis & Weakness of Rotator Cuff-> Sholder Protraction. Changing Length/Load in Supraspinatus -> Constant OverLoad-> ....
Evidence:
Боль в плече месте прикрепления и локте.
Тяжело поднимать руки в coronal plane.
Очень тяжело поднять руку на уровне головы.
При наличии tr.points тяжело сделать contraction in short range.
Clicking in joint <- tight supraspinatus squeeze joint surfaces
Palpation: Руку на Scapula Spine. Поднятие руки 45 градусов между sagital & coronal planes. Почувтвуется лекое движение, натяжение под пальцем.
Учавствует во всех движениях с поднятием руки. Даже при болтании рукой при ходьбе. Держание портфеля в руке.

Reasons:
Dynamic: Wrong movenent: Поднятие тежестей, долгое держание руки на весу.
Kinetic: tight Pectoralis & Weakness of Rotator Cuff-> Sholder Protraction. Changing Length/Load in Supraspinatus -> Constant OverLoad-> ....
Evidence:
Боль в плече месте прикрепления и локте.
Тяжело поднимать руки в coronal plane.
Очень тяжело поднять руку на уровне головы.
При наличии tr.points тяжело сделать contraction in short range.
Clicking in joint <- tight supraspinatus squeeze joint surfaces
Поза дерева Цигун & Работа с компьютером
Основная идея. Работать за компьютером в позе Дерева Цыгун.
Поставил компьютер на уровне локтей в положении стоя. Далее принять позу дерева из Цигун.
Слегка согнуть колене выпрямить спину. Руки согнуть в локтях как будто охватил шар или ствол дерева. В этом положении можно очень долго находиться без вреда для здоровья.
Поставил компьютер на уровне локтей в положении стоя. Далее принять позу дерева из Цигун.
Слегка согнуть колене выпрямить спину. Руки согнуть в локтях как будто охватил шар или ствол дерева. В этом положении можно очень долго находиться без вреда для здоровья.
Weakness -> Immobilization in short range.
Прочитал пару страниц из книги UMN Sindrom. Несколько интересных идей от туда:
Spastisity - impairment when stretch reflex become velocity dependent. Например если резко мышцу вести через ROM то она будет слегка напрягаться.
Hypertonus - повышенная сопротивляемость мышцы пассивному растяжению. Те мышца как бы здоровая (not chronic roped) но не вполне расслабленная и более упругая чем должна быть.
Tonus - сопротивляемость упругость на растяжение, может быть active & passive.
Contraction - сокращение мышцы. Может быть voluntary & involuntary.
Stretch reflex: 1) phasic быстрый рефлекс
a) spindels stretched ->Ia receptors &
b) fast stretching -> tendon percussion (сотрясение) -> spindels stimulation
radiating stretch reflex: percussion передается в соседние мышцы
tendon percussion massage technique produce reflex light contraction, can be used for relaxation or stimulation.
Muscle weakness + overuse -> immobilization in short range (closed-short state) -> changes in tone: hypertonus, tightness-> decreased circulation -> contraction -> tissue changes (fibrosis, adhesion, myofasciatis etc)
Immobilization in short range -> degeneration, lose of muscle mass
Overuse: reppetive -> weakness, spasticity
overtrain -> hypertonus, overdevelopment
Repetitive overuse - lock in short range, spasticity, proprioreceptors overexcitement
Overuse: reppetive -> weakness, spasticity
overtrain -> hypertonus, overdevelopment
Repetitive overuse - lock in short range, spasticity, proprioreceptors overexcitement
Proper amount of stretch per day: at lease one time carry through ROM
TIGHT-Short/Long-WEAK; Short/Long-LOCKED STATE.
Muscle tightness is defense from unstable-dangerous state.
Weakness-> overuse->disability
------------------------------------------------------------------------------------------------
Tight ~ Roped [osteopatic]
Disfunction - состояние характеризующееся неправильным выполнением функции,
более применимо к joints или группе мышц.
Somatic dysfunction [osteopatic] - более общее понятие. можно описать
TART: tenderness; assimetry; restriction; tissue changes
Disability [physical therapy] - состояние бессилия неспособности,
более применимо к отдельной мышце,
последствие muscle weakness
Weakness-> overuse->disability
Muscles. Tight-weak & Tight-Strong.
TIGHT-SHORT MUSCLES.
Short-Locked State.
Repetitive overuse
Short-Locked State.
Repetitive overuse
Reasons:
1) Weakness->Защита от переиспользования. Реакция на боль
2) overuse{ repetetive movements (phasic muscles),
constant escentric load (tonic posturalmuscles) }
->Weakness
-> Lock in Sort range - Защита от дальнейшего переиспользования
Symptoms:
Chronic, roped, Tissue changes, nodules,
tendons stress ->tendons changes, calsification, inflamation
Treatment:
1) Massage middle part: straight & perpendicular strokes long-deep strokes,
tendons deep cross
tendons deep cross
friction.
2) Strengthening for elongation: a) midle-long range isotonic exercise
b) isometric in long range
Examples:
Psoas, QL
Psoas, QL
TIGHT-LONG-WEAK
Long-Locked State
Constant ascentric load
Ressons: constant ascentric load
Examples:
Multifidus, Supraspinatus
postural muscles
Treatment:
Manual: Counterstrain, Gentle Massage ,
Exercise: Strengthening-Shortening: short isotonic, isometric in short rom
Long-Locked State
Constant ascentric load
Ressons: constant ascentric load
Examples:
Multifidus, Supraspinatus
postural muscles
Treatment:
Manual: Counterstrain, Gentle Massage ,
Exercise: Strengthening-Shortening: short isotonic, isometric in short rom
TIGHT-STRONG MUSCLES
TODO:
Может ли быть strong short muscle? - думаю да если закачать в short range.
Может ли Muscle быть Tight-strong? - да может. Пример: belly dancers - спина, calves; спортсмены
Как это будет выглядеть? - bumped, hypertonic, overdeveloped
Какие причины? - overtrain + overuse
------------------------------------------------------------------------------------------------
Tight ~ Roped [osteopatic]
Disfunction - состояние характеризующееся неправильным выполнением функции,
более применимо к joints или группе мышц.
Somatic dysfunction [osteopatic] - более общее понятие. можно описать
TART: tenderness; assimetry; restriction; tissue changes
Disability [physical therapy] - состояние бессилия неспособности,
более применимо к отдельной мышце,
последствие muscle weakness
понедельник, 14 марта 2011 г.
Hip joint ligaments или не все так просто как кажется
Недавно у меня сформировалась теория kinetic chain, muscle antagonist agonist pattern etc
Но видимо не все так просто в человеческом организме. Моя модель затрагивает только мышечную систему. А ведь еще есть связки фасция и самое сложное - нервы.
По поводу моего кейса Лев Калика DC говорит что у меня слабость связок воркруг trocanter причем я не совсем понял гле именно. Поэтому он двигается не так как положено, вокруг возникает постоянное напряжение. Это кажется весьма логичным поскольку боль концентрируется в ягодичной области а напряженность в QL вторична. Также я просыпаюсь утром с stifness. Возможно это следствие манипуляций гребнева и других умельцев как в случае с Дорейн. Возможно последствия травм дзюдо. Отсяда вытекает Pelvis Obliquency. тк разное положение femur head то распределение сил на Inominate bones получается разное. Также из-за разной траектории движения при ходьбе возникает ассиметрия мышц. Также при слабости Glut Max основыным hip extensor становится hamstring. Из-за разного пркрепленяия и разных векторов сил создающих накгузку на связки и сустав, hip joint начинает разбалтывать что в результате ведет к osteoartritis.
Что вызывает боль? - Сидение на стуле и любая флексия бедра выше 90 градусов. Поднимать ногу выше 90 тяжело. Лежание с ногой 90. IliaPsoas выглядит как слабый в этом положении. Хотя Situps я делаю лекго. Возник вопрос Почему остальные упражнения на psoas делаются лекго а сидя поднимать колено вверх тяжело? Возможно тут больше работает Iliacus ? Или мешают tight gluteus? В теории MAT считается что надо находить положения нестабильности и делать contraction в положении нестабильности. Но что если нестабильноее положении опасно и тело таким образом защищается делая это положение труднодоступным? После выполнения серии упражнений с весом на флексию бедра из положения сидя боль увеличилась.
Еще вопрос. Лев Калика что-то сказал что Psoas дает стабильность при слабости передней части femur head. Я думаю у меня проблема скорее в задней. Это вытекает из положения вызывающего болевой синдром. Это можно объяснить слабостью Gluteus Maximus которые обеспечивают стабильность femur в posterior part. Лежание на животе тоже вызывает боль что не совсем понятно.
Как лечить. Видимо надо укреплять Gluteus max и может быть Psoas.
Вобщем есть над чем задуматься.
Но видимо не все так просто в человеческом организме. Моя модель затрагивает только мышечную систему. А ведь еще есть связки фасция и самое сложное - нервы.
По поводу моего кейса Лев Калика DC говорит что у меня слабость связок воркруг trocanter причем я не совсем понял гле именно. Поэтому он двигается не так как положено, вокруг возникает постоянное напряжение. Это кажется весьма логичным поскольку боль концентрируется в ягодичной области а напряженность в QL вторична. Также я просыпаюсь утром с stifness. Возможно это следствие манипуляций гребнева и других умельцев как в случае с Дорейн. Возможно последствия травм дзюдо. Отсяда вытекает Pelvis Obliquency. тк разное положение femur head то распределение сил на Inominate bones получается разное. Также из-за разной траектории движения при ходьбе возникает ассиметрия мышц. Также при слабости Glut Max основыным hip extensor становится hamstring. Из-за разного пркрепленяия и разных векторов сил создающих накгузку на связки и сустав, hip joint начинает разбалтывать что в результате ведет к osteoartritis.
Что вызывает боль? - Сидение на стуле и любая флексия бедра выше 90 градусов. Поднимать ногу выше 90 тяжело. Лежание с ногой 90. IliaPsoas выглядит как слабый в этом положении. Хотя Situps я делаю лекго. Возник вопрос Почему остальные упражнения на psoas делаются лекго а сидя поднимать колено вверх тяжело? Возможно тут больше работает Iliacus ? Или мешают tight gluteus? В теории MAT считается что надо находить положения нестабильности и делать contraction в положении нестабильности. Но что если нестабильноее положении опасно и тело таким образом защищается делая это положение труднодоступным? После выполнения серии упражнений с весом на флексию бедра из положения сидя боль увеличилась.
Еще вопрос. Лев Калика что-то сказал что Psoas дает стабильность при слабости передней части femur head. Я думаю у меня проблема скорее в задней. Это вытекает из положения вызывающего болевой синдром. Это можно объяснить слабостью Gluteus Maximus которые обеспечивают стабильность femur в posterior part. Лежание на животе тоже вызывает боль что не совсем понятно.
Как лечить. Видимо надо укреплять Gluteus max и может быть Psoas.
Вобщем есть над чем задуматься.
четверг, 10 марта 2011 г.
Patterns of muscle antagonism & synergism.
Joints & competitive muscle groups.
Joints & synergetic muscle groups.
Synergism. Пусковые muscle. Key/muscles. Initial muscles. Kinetic chain disruption.
Joints & synergetic muscle groups.
Synergism. Пусковые muscle. Key/muscles. Initial muscles. Kinetic chain disruption.
Neiro-Muscular Self Release Technic
effective manual techniques: MET, PNF, ART/orthopedic massage, AIS
effective exercise systems: NASM, Yoga, MAT
Combination of ART & PNF & AIS => Isolated combined Exercise with Activation Inhibited muscle (isometric ,concentric contraction) and Inhibition Hyperactive antagonist group of muscles muscle (pressure) =>Neiro-Muscular Self Release Technic
TODO: развить теоритически описать протокол, запотентовать сделать видео на youtube.
effective exercise systems: NASM, Yoga, MAT
Combination of ART & PNF & AIS => Isolated combined Exercise with Activation Inhibited muscle (isometric ,concentric contraction) and Inhibition Hyperactive antagonist group of muscles muscle (pressure) =>Neiro-Muscular Self Release Technic
TODO: развить теоритически описать протокол, запотентовать сделать видео на youtube.
Подписаться на:
Комментарии (Atom)